Cancers after the age of 75
Elderly cancer patients have always existed. Now there are more of them than before, as people are living longer. Therefore, special attention must be paid to the treatment of older cancer patients.
Riikka Huovinen
Elderly cancer patients have always existed. Now there are more of them than before, as people are living longer. Therefore, special attention must be paid to the treatment of older cancer patients.
Riikka Huovinen
The increase in cancer cases in recent years is largely due to the fact that people live longer. The risk factors for the most common cancers have a long time to impact and increase the risk of disease in older people.
Age does not usually restrict the active treatment of cancer, but the patient’s other diseases and poor general condition do. Geriatric and psycho-social assessment of the patient’s situation help in making the treatment decisions.
Cancer surgery can usually be carried out normally, regardless of age. Adjuvant therapy reduces the risk of relapse and spreading of the cancer, so they are also considered as alternatives for the elderly. Radiation therapy and cancer drug disadvantages in advanced cancer are considered carefully in relation to the anticipated benefits, in particular quality of life.
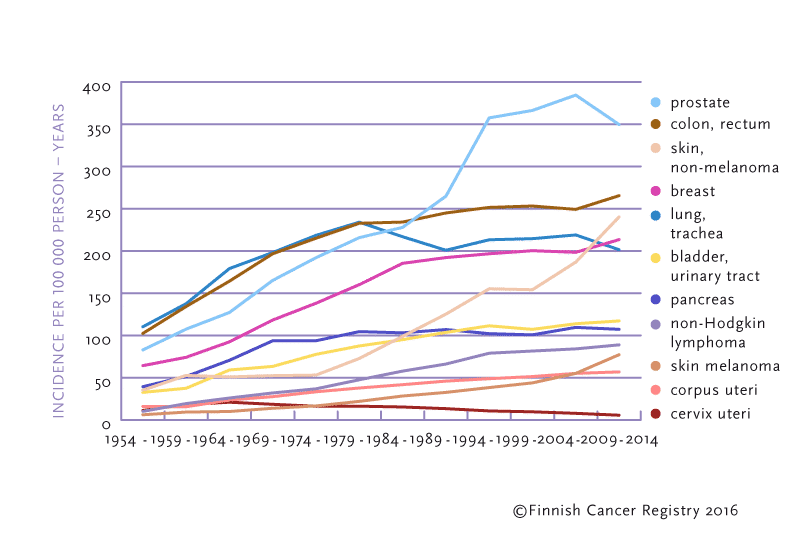
Figure 1. Trends in cancer incidence in persons aged 75 or older in 1954–2013.
In Finland, already more than 32 000 new cancers were found in 2013. The amount is threefold compared to the incidence rates in the 1970s. [1] The main reason for the increase in the incidence of cancer is that people live longer than before.
A person’s average lifespan has continuously extended. Life expectancy is most affected by deaths in childhood or during working age. In particular decreases in infant mortality extend the life expectancy of the entire population. In Finland, the health of the population began to improve rapidly after the war, as education and income increased.
The life expectancy for Finnish men is currently 79 years and for women 84 years. [2] The maximum age in humans is thought to be between 115 and 125 years.
Many of the elderly are independent and in good condition, and have an active life. Falling ill with cancer is a shocking experience regardless of age, and most of the elderly wish for active treatment, if such is available.
In 2013, around 5 700 cancers were found in men over 75 years of age, which is 34% of all new cancer cases in men. In the same year, about 5 500 cancer cases were found in women over the age of 75, representing 35% of all new cancer cases in women. The Finnish Cancer Registry forecasts that in 2025, about 9 500 cancers in men and about 8 500 cancers in women over the age of 75 will be diagnosed. The growth in the number of cancer cases caused mainly by aging is significant. Accordingly, special attention must be paid to the treatment of elderly cancer patients.
The most common cancers in older men are prostate, lung, and gastrointestinal cancers. The most common cancers in older women are breast, gastrointestinal, lung, and gynecological cancers. [1]
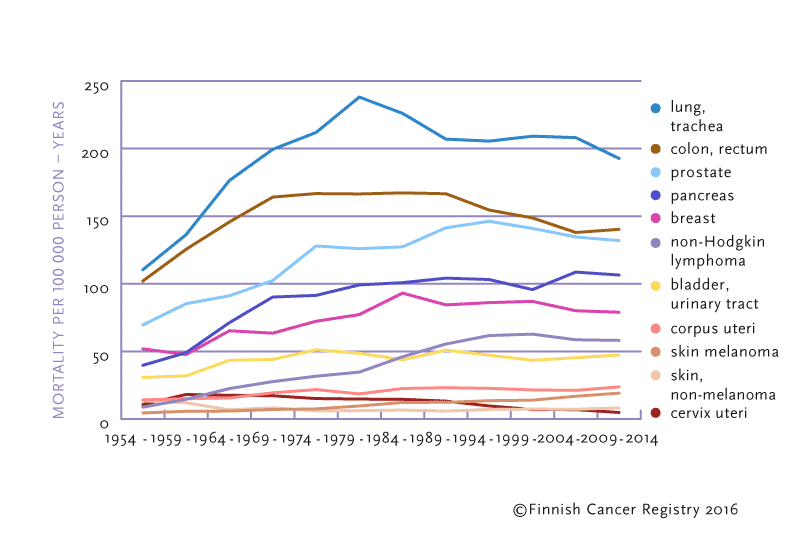
Figure 2. Trends in cancer mortality in persons aged 75 or older in 1954–2013.
Cancer is the most common cause of death in the world and the second most common in Finland. [3] In Finland, it remains more common to die from cardiovascular diseases, even though mortality caused by cardiovascular diseases is decreasing.
Every fourth death in Finland is caused by cancer. Compared with other Nordic countries, cancer causes relatively less mortality in Finland.
Lung cancer is the most common fatal cancer in men over 75 years of age. The second most common is prostate cancer and the third is pancreatic cancer. In women over 75 years of age pancreatic cancer is the most common fatal cancer, the second most common is lung cancer and the third is breast cancer. [1]
Of skin cancers, particularly basal cell and squamous cell carcinomas often occur in the elderly, but they do not cause mortality.
The average five-year survival ratio in patients diagnosed with cancer at 75 years of age or older is 61% in men and 53% in women. Men’s larger survival ratio is primarily due to the fact that prostate cancer, which has a relative survival ratio of nearly 90%, is common among elderly men. Only 56% of prostate cancer patients, however, are alive after five years, because many die of causes other than cancer. In particular, the survival in non-Hodgkin lymphoma, prostate cancer and skin melanoma has increased in the 2000s (Figure 3).
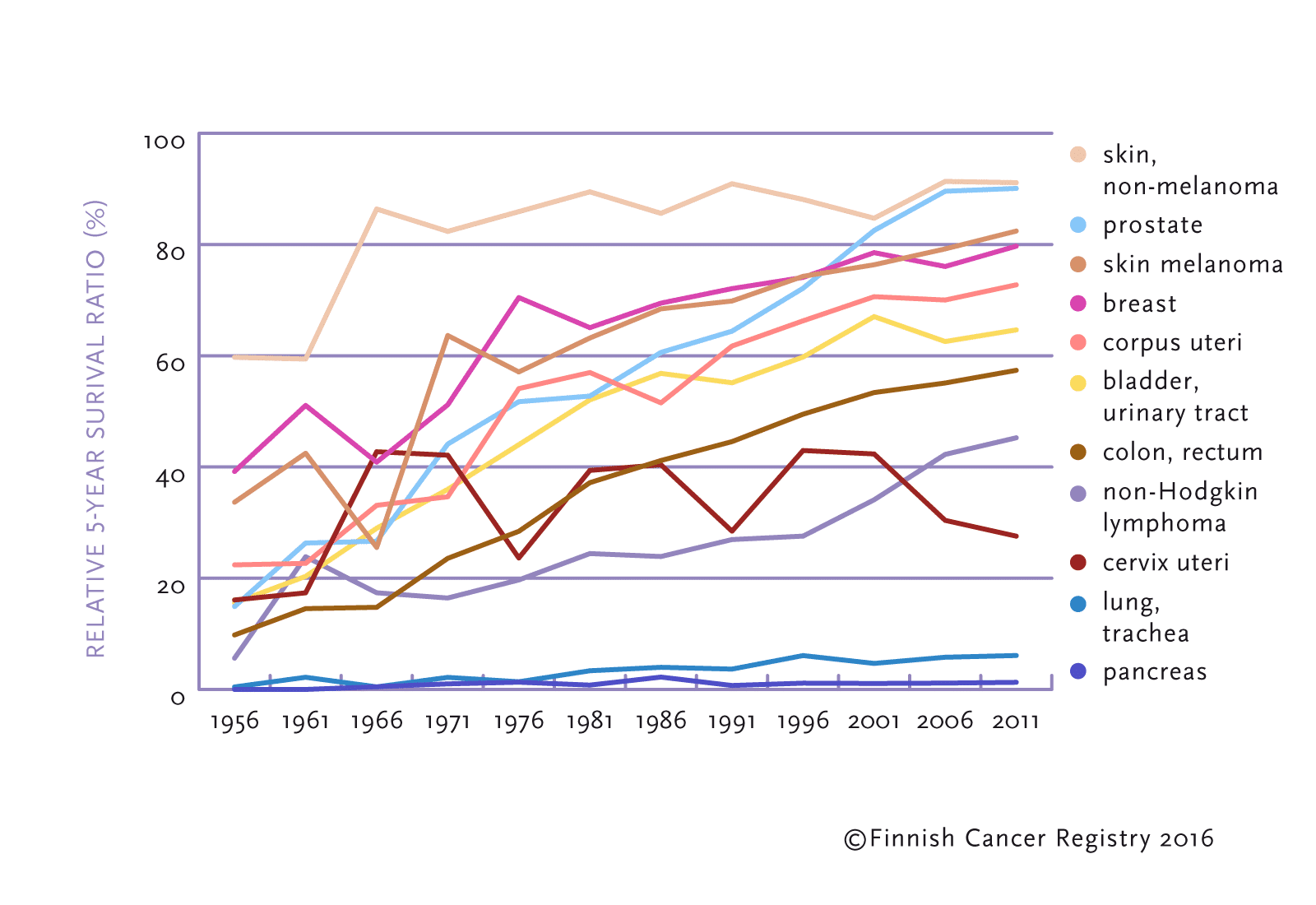
Figure 3. Trends in relative five-year survival ratio for cancer patients diagnosed at 75 years of age or older in 1954–2013.
Age in itself significantly increases the risk of cancer. Also other risks associated with lifestyle accumulate in the elderly. However, it is never too late to make healthy lifestyle changes. Thus quitting smoking, limiting alcohol use, favoring a vegetable-rich diet, weight control, and physical activity may all be recommended to the elderly.
A healthy lifestyle improves overall health comprehensively, which helps older people maintain better well-being. Good general condition and muscle strength, independence, as well as controlled diabetes and blood pressure can decisively work in favor of active treatment, if the patient is for example about to have a large operation of the abdominal cavity or lungs, and removing the cancer completely would be possible.
Cancer found in its early stages is usually curable by surgery and adjunctive therapy, regardless of the patient’s age. [4] Therefore, early cancer diagnosis is important also in the elderly. Even though a patient is very old and has other diseases, early-stage cancer can often be operated. Surgery may improve the patient’s quality of life, even if the aim is not to extend the patient’s life span. [5] Particular care is placed in evaluating the elderly’s eligibility for operations. Radiation and medical treatments provided after surgery reduce the risk of cancer spreading. These adjuvant treatments may cause temporary harms, but in spite of them it is easier for elderly patient to live with other illnesses without metastatic cancer. Many special features are associated with the treatment of cancer in the elderly. Little research exists on antitumor and radiation treatments for the elderly, as most clinical trials have not included patients over the age of 65. [6] Hence for example chemotherapy has been avoided in treating patients that are over 65. In radiotherapy, in turn, smaller dosages than usual may have been used. [7]
Current treatment practices are based on subgroup analyses of studies, or recommendations made by experts, and not necessarily on randomized trials. In recent clinical studies patients generally no longer have upper age limits, but patients are selected according to their general condition, so that other diseases have been ruled out, and the activity of kidneys, liver, heart and lungs are within normal limits. Therefore, we are gradually also starting to accumulate data on the treatment of elderly cancer patients. Oncological treatments such as chemotherapy and radiotherapy generally cause more harm for the elderly than for the younger. These harms are also more serious in elderly patients. On the other hand, biological age does not necessarily reflect the patient’s possibilities to cope with e.g. adjunctive chemotherapy. If the patient does not have other diseases, the treatment plan may at least in the beginning be prepared in the same way as for younger patients. The effect of drug treatments and radiotherapy is likely to be the same regardless of age.
Other diseases in the elderly–such as diabetes, vascular disease, and impaired renal function–increase the risk of infections, anemia, nausea, depression and exhaustion. [8] Elderly patients also recover from treatments more slowly. A few weeks bedridden may impair the general condition of the elderly so that they might no longer fully recover. To find the equilibrium between the benefits and disadvantages of the treatment of the elderly, over-treatment and under-treatment need to be balanced.
Effective chemotherapy should be started in spite of the expected harms in the elderly patients, for example, in the treatment of aggressive lymphoid tissues if healing is possible on the basis of earlier data. [9] Supportive treatments help in carrying out chemotherapy.
Geriatric and psycho-social assessment With long-term cancer treatment it is often important that the patient receives support and care from loved ones. If the patient does not have close friends or family, carrying out the treatment may be difficult or even impossible. The geriatric and psycho-social assessment made prior to treatment help in selecting proper therapy. They are particularly essential when symptomatic treatment is selected.The patient’s remaining life span can be evaluated according to how independently she or he will perform daily activities, how many other diseases she or he has in addition to the cancer that requires treatment, and what her or his nutritional status is. [10]
Dementia and memory disorders may prevent treatment because cancer treatment requires understanding and cooperation skills. The patient must also have a positive stand on the treatment, because no one can be treated against their will.
The patient has the right to participate in the selection of the treatment method whenever there are alternatives, and also to refuse offered treatment. If the patient refuses active treatment, she or he will be offered good symptomatic treatment and follow-up.
Cancer diagnoses may cause deep depression in the elderly, which may result in a false impression of them giving up on their own health issues. The patient may refuse e.g. surgery on breast cancer, even if it would be an easy and safe operation. The identification and treatment of depression, as well as starting active cancer treatment can significantly improve the patient’s quality of life, even if this would not extend their life.
The average age of prostate cancer patients is about 70 years. Roughly one-third of prostate cancer diagnoses are given to patients over the age of 75. Prostate cancer usually grows slowly, and approximately 90% of patients are alive five years after the diagnosis. According to studies, latent, asymptomatic prostate cancer occurs in even up to approximately 60% in men over the age of the 80. [11] However, prostate cancer is the second most common cause of cancer mortality within the age group of over 75 years. [1] If the cancer is confined to the prostate and has not spread more widely, extensive surgery or local radiation therapy will be considered as treatment. [12] Surgical technology and the technical implementation of radiation therapy have evolved in such a way that the severe complications caused by them, such as urinary and bowel function related problems, have been reduced. Surgery requires the patient to be in better general condition than radiation therapy, and thus radiation therapy is often selected for treating elderly patients.
Metastatic prostate cancer, in turn, is treated with hormone therapy, which may keep cancer spread to the bones asymptomatic for many years. Chemotherapy treatments require the patient to be in fairly good general condition, so they are not suitable for very elderly or patients with multiple diseases. Hormone therapies do not result in sudden and severe harm, but may be associated with osteoporosis, sweating, loss of muscle tone and increased cardiovascular disease risk. [13]
Lung cancer is still one of the cancers with the worst prognosis, and smoking is its main risk factor. The decrease in men’s smoking is visibly seen in the reduction of lung cancer cases. Surgery is a curative treatment for early-stage lung cancer. It is, however, only rarely possible, and the poor functioning of the heart or lungs of the elderly patient may prevent the surgery. Local radiation therapy can be used to relieve the symptoms of lung cancer, regardless of age. Chemotherapy treatments for lung cancer are quite severe and their effectiveness weak, so they are rarely given to elderly patients.
In recent years, new biological medicines have become available on the market, and they are used in the treatment of certain rare types of lung cancer.
The most common intra–abdominal cancer is colon cancer, which today has a good prognosis. Intestinal disorders are common in older people, and therefore they may be left unexamined. On the other hand, emphasis is currently placed on the active investigation of elderly patients with intestinal symptoms, because the risk of cancer increases significantly with age. The risks related to surgery of the abdominal cavity are significant. Therefore, symptomatic treatment may be settled with in cases where patients have other serious illnesses, such as heart failure. Colon and rectal cancer surgery also improve the quality of life of the elderly patient, even if the surgery would not prevent the progression of metastases outside the intestine. [5] Chemotherapy is used as adjuvant therapy after colon cancer surgery. Adjuvant treatments cannot be performed if the patient has other medical conditions and multiple other medications. However, chemotherapy given as tablets may be suitable for the elderly patients with no heart disease. [14] Advanced colon cancer treatment has a number of medicinal options. Chemotherapy treatments and biological drugs delaying cancer progression and relieving the symptoms may also be considered in elderly patients. It is important to always anticipate the potential harm for the heart or the kidneys.
Breast cancer in the elderly is rarely a biologically aggressive subtype, yet nevertheless the mortality rate of breast cancer in older people is greater than in younger people. One reason for this is the fact that the cancer has often advanced more widely in elderly patients at the moment it is diagnosed. In breast cancer, the prognosis is especially good if it is diagnosed at an early stage. Breast cancer can usually be operated normally, regardless of age. Armpits are examined by sentinel node scanning, which poses no risk to the patient. A breast can be removed even under local anesthesia. Breast-sparing surgery is usually supplemented by radiotherapy. In the past, it was a customary to remove the entire breast of an elderly patient on a much more lightly basis in order to spare them from radiotherapy. Today, radiation therapy may be provided in a short, three-week treatment cycle, instead of the previous five-week cycle. Active Breathing Control technique also enables minimizing the radiation dose received by the heart. Today, the advantages and disadvantages of mastectomy and breast-saving surgery can be contemplated together with the elderly patient. Adjuvant treatments are also used after the surgery, which reduces the risk of breast cancer recurrence. A five-year hormonal drug therapy with tablets can usually be started for older patients. [15] There are many options in chemotherapy, and they may be considered also on the basis of the biological subtype of breast cancer. If the breast cancer has spread, hormonal drugs can slow down its progression and relieve symptoms. There are a number of different chemotherapies, and they are administered individually. [14] However, the disadvantages of chemotherapy, such as anemia, mucous membrane irritation and fatigue, are often worse than the symptoms caused by cancer, especially if the pain is controlled with pain medication.
The services of cancer organizations are intended for everyone who is thinking about issues related to cancer.
Chat conversation
You can chat with a nurse specializing in cancer – Cancer organizations’ chat service is available on the kaikkisyovasta.fi website from 9 am to 3 pm.
Free phone consultation
The helpline is available at 0800 19414. The nurse answers the phone on Mondays and Thursdays from 10 a.m. to 6 p.m. and on Tuesdays, Wednesdays and Fridays from 10 a.m. to 3 p.m. The service is free of charge.
Regional services
Find your nearest regional association or national organization that will help you move forward when you need support and help.